
")

Super User
Ovulation Induction (OI)
Ovulation Induction (OI) is the controlled administration of drugs to stimulate the ovaries to produce mature eggs. OI is typically applied to couples in which the woman has irregular menstrual cycles and in which investigations indicate that they may not be ovulating on a regular basis.
Two types of fertility drugs are commonly used in OI:
Clomiphene Citrate: often called Clomid. This drug is an anti-oestrogen and works by stimulating your body into releasing more Follicle Stimulating Hormone (FSH). These higher levels of FSH stimulate the ovaries to produce eggs. Clomid is usually given at the beginning of the menstrual cycle for 5 days. The mature egg is normally released (ovulation) naturally. However, ovulation can also be triggered using by a single injection of human Chorionic Gonadotrophin (hCG).
Gonadotrophin: such as Menopur, Gonal F & Puregon. These drugs are usually given daily to stimulate the development of a single mature follicle. Again, the mature egg is ovulated or the ovulation can be stimulated by hCG.
Ultrasound scans and blood tests are performed to ensure that OI is both safe and effective. Once a mature follicle has been produced you will be advised when the best time for intercourse is in order to help achieve a pregnancy. Typically, couples need only a few months of OI in order to conceive.
Birth Defects
It is important to remember that any medical or surgical treatment has risks, adverse effects and side effects. Couples should be aware that one baby in 20 born worldwide will have a birth defect. There is no clear evidence that infertility medicines, if properly used, increase this risk.
Cancer
Breast Cancer
Of the cancers of the sex organs, breast cancer is most common, occurring in one in eight Barbadian women.
The cause, or aetiology of breast cancer is unknown. Various factors or diseases make breast cancer more likely. Breast cancer in a mother or sister increases the risk, as does some types of non-cancerous (benign) breast lumps.
Breast cancer is more common in infertile women. Some medical research suggests that cigarette smokers are at increased risk.
Monthly breast self-examination is recommended for all women. All lumps should be investigated immediately. Most breast lumps are benign.
There is no screening method for breast cancer, although mammography detects small cancers.
Ovarian Cancer
Occurs in about one in 90 women. Its aetiology is also unknown.
May also occur in families in 10-15% of cases.
It is more common in infertile women.
The oral contraceptive pill decreases the risk of cancer of the ovaries. This remarkable advantage of "The Pill" occurs, not only while the woman takes The Pill, but also for at least five years after stopping The Pill. There is no effective screening method for ovarian cancer. Every woman is advised to have a gynaecological examination and "Pap Smear" every two years to minimise the risk of ovarian, uterine and cervical cancers going undetected.
Cervical Cancer
The lifetime risk of cervical cancer is one in 95 women.
Cervical cancer can be screened by cervical cytology, by the Pap smear.
The aetiology of cervical cancer is related to sexual activity. For this reason, every woman having sexual intercourse should have a Pap smear every two years. An increased number of sexual partners and a papilloma or wart virus infection can also increase the general risk of development of cervical cancer.
A Pap smear every two years, as well as regular gynaecological and breast examinations, are currently the best methods to prevent or detect women's cancers.
Cancer After Infertility and IVF
Doctors have used fertility drugs worldwide since the 1960s, triggering women's ovaries to produce eggs. This approach proved successful in assisting many women with fertility problems to become pregnant and have children.
In the past 20 years the use of fertility drugs has increased markedly following the development of IVF.
Findings of an Australian Study relating to incidence of Cancer and IVF.
Background
The growth in the number of women seeking help to become pregnant provided an opportunity for a study, the largest of its type anywhere in the world.
The study followed up 29,700 women referred to any of ten participating Australian IVF clinics between 1978 and 1993. Of this total:
20,656 women received fertility drugs during IVF (the "treated group")
9,044 women referred for IVF did not end up having fertility drug treatment (the "untreated group").
Depending on the year that women joined an IVF program, the duration of follow-up ranged from one to 22 years, with the majority followed up for five to ten years.
This study was conducted to address concerns that the use of fertility drugs might be associated with an increased risk of cancer.
Study's Aims
To see whether there was any increase in the number of cancers of the breast, ovary and uterus in women on IVF, compared with the number expected among women of the same age, followed up over the same period in the general population.
In the event that there were more of these cancers than predicted, how this might be explained.
Findings
The major finding was that cancers of the breast and ovary were no more common in IVF patients overall than in the general population. Of 29,700 who joined IVF programs, researchers predicted 155 breast cancers and found 143. For ovarian cancer, 13 cases were predicted and 13 were found.
Cancers of the uterus were more common than predicted in untreated IVF patients but were no more common than predicted in the treated group. (Among the 9,044 women in the untreated group, three cases were predicted and seven found).
More women than predicted in the treated group had breast cancer diagnosed in the first year after treatment with fertility drugs. This finding disappeared with time and is discussed below. (Among the 20,656 women, 9 breast cancer cases were predicted in the first year after treatment and 17 were found.)
Women with unexplained infertility had a significantly higher incidence of ovarian and uterine cancer, whether or not they were exposed to fertility drugs, than the general population. (Out of 3,800 women with unexplained infertility, two cases of ovarian cancer were predicted and five were found. With regard to uterine cancer, one case was predicted and five were found).
There was no evidence of any link between the number of treatment cycles or type of fertility drug used and increased cancer incidence. Changes in the types of drugs used in IVF and the amount of ovarian stimulation do not appear to have had an overall impact on cancer in participating women.
Conclusions
The findings provide reassurance that the incidence of breast and ovarian cancers in IVF patients are the same as that for women of the same age in the general population when considered over a five to ten-year period.
The evidence of increased numbers of cancers above, predicted in small numbers of women, in particular subgroups, needs further study. While there was no overall increase, the occurrence of above expected numbers of breast cancer in the first year after treatment is consistent with other research showing a small increase in diagnoses of breast cancer shortly after women give birth. The same effect has been seen in recent users of The Pill and hormone replacement therapy. Possible explanations for this finding after IVF treatment include earlier detection of abnormal breast changes due to close medical supervision, the biological effects of fertility drugs, or both.
Explanations for the relationship between unexplained infertility and the increase in ovarian and uterine cancers are harder to come by but research is continuing. In a bid to explore such issues, the research team has started a more detailed investigation of about 700 IVF patients, some of whom have cancer and others who do not.
Summary
The risk of cancers in women is best reduced through regular women's health check-ups, breast examination, Pap smears and gynaecological examinations - and by the use, at other times, of The Pill. The most effective way of minimising the risk of breast and ovarian cancers in infertile women is to help them to have a baby. However, the study does reinforce the importance of women having medical check-ups at regular intervals after fertility treatment.
Multiple Pregancy
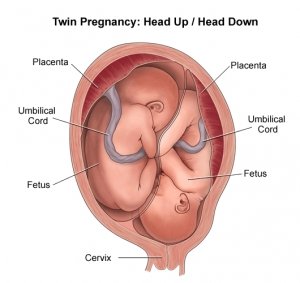
Management of IVF in our clinic, is characterised by a conservative approach to embryo transfer, in order to reduce the likelihood of multiple births. Generally between one to three embryos are transferred in each attempt, depending on the individual patients history.
Although the world's first IVF baby was born from a natural cycle with spontaneous ovulation, controlled ovarian hyperstimulation is now the norm. Consequently, multiple pregnancy has become common, and it has been estimated that in total, 45% of IVF babies born are from multiple pregnancies, with twinning rate of nearly 25%, triplet rate of 2-3% and quadruplet rate of 0.5% of pregnancies worldwide.
Unfortunately, neonatal and perinatal mortality rates are 3 to 6 times higher for twins when compared to singleton births, and 5 to 15 times for higher order multiples, and the risk of cerebral palsy is six times higher for twins, and twenty times higher for triplets. Multiple pregnancy also places greater physical strain on the mother, with an increased incidence of miscarriage, high blood pressure, bleeding during pregnancy, increased risk of vomiting during pregnancy, and premature birth.
The complication of being born prematurely includes difficulty with breathing, higher incidence of jaundice, and feeding difficulties. Twins also have a higher incidence of congenital abnormality. Triplets are almost always delivered by Caesarean section, and twins far more often. Even if the babies are born normal, caring for two, three or more babies can be a challenge, with extra emotional, physical and financial stresses.
To reduce the risk of multiple pregnancies we have to limit the number of embryos transferred. In deciding how many embryos are to be transferred, we need to consider the number of previous pregnancies, woman's age, the duration of infertility, the reason for the fertility problem, the number of previous attempts, the number of fertilised embryos, and the cleavage stage and quality of embryos replaced. Excess embryos that are of good quality can be frozen, stored, and used in a subsequent cycle, if necessary.
Ovarian Hyper Stimulation Syndrome (OHSS)
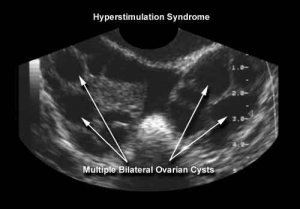
Women contemplating ovarian stimulation should be aware that the procedure carries risks that are comparable with the risks of elective surgery.
All women undergoing ovarian stimulation, such as during an IVF treatment cycle, experience enlargement of their ovaries and a complex change in their hormone balance. The condition is often marked by weight gain, as excess fluid is retained. For this reason it is important to note your weight at the beginning of each IVF cycle.
For up to 5% of stimulated women this can be quite unpleasant with abdominal bloating and pelvic discomfort, however, for <1% of stimulated women, the abdominal pain and fluid retention is so severe that admission to hospital is necessary. Symptoms may include marked abdominal swelling, nausea, vomiting and diarrhoea, lower abdominal pain, and shortness of breath. Hyperstimulation varies in severity and rarely requires treatment in hospital, but you must contact the clinic if you notice any of the above symptoms so that we can monitor you closely.
"Ovarian Hyperstimulation Syndrome" (OHSS), usually presents a few days after embryo transfer; symptoms being provoked by the hCG injection (Pregnyl/Profasi).
Severe symptoms require:
- bed rest
- correcting the fluid imbalances with an intravenous drip
- relieving pain and nausea
- Injections of heparin to counter the tendency of the blood to clot abnormally.
Fortunately this condition is self-limiting. It usually resolves after several days, with a natural excretion of the abnormal accumulation of fluid, however it may persist for weeks, especially if a pregnancy has been achieved. Once the condition has resolved the pregnancy can be expected to proceed normally.
On RARE occasions very serious complications have been associated with OHSS:
1. Abnormal blood clotting has caused strokes
2. Blood clots have migrated to the lungs, a complication that can be fatal
3. Enlarged ovaries can twist or bruise, requiring surgery
4. Weeping of fluid into the abdomen may be accompanied by a similar collection of fluid about the lungs and heart, interfering with their proper function
5. Liver or kidneys may stop working effectively.
There have been individual case reports of blood clotting and stroke complications of severe OHSS. One and a half million IVF babies have been born world wide with only four deaths that have been reported in world medical literature.
Age and Fertility

The number of couples in their late 30s and 40s attempting pregnancy is increasing. Currently 25% of patients at Barbados Fertility Centre are aged 40 or over. It is common to delay starting a family for a number of reasons: second relationships, career and educational demands, desire for financial stability, waiting for a stable relationship, however it is important to understand that fertility in women declines with age, particularly in the late 30s and 40s. This is a normal part of the ageing process.
As women become older, the chance of becoming pregnant is lower, the chance of having a miscarriage is higher and there is an increased risk of chromosomal abnormalities in the baby. In the general population, the chance of becoming pregnant after the age of 40 is estimated to be only 5% per cycle compared to about 25% per cycle in the under 40 age groups. One-third of couples where the woman is over 35 may have fertility problems. Treatments such as IVF cannot reverse the effects of age on fertility.
As men become older, the chances of achieving a pregnancy are lowered to a lesser degree than in women, as sperm generation continues throughout life. Women, on the other hand, are born with a finite number of eggs and do not produce any more during a lifetime. Geneticists believe genetic mistakes do increase with age in males. This is thought to be in the order of 0.5% in males over 40 years of age and increases to 1% at 45, 2% at 50 and 5% at 55.
Reasons for Decline in Fertility
There is an increased incidence of gynecological problems as women age. Endometriosis, fibroids, and pelvic infections all may reduce fertility, however the ageing of the eggs is thought to be the major cause of reduced fertility. Girls are born with about 400,000 eggs in their ovaries. The eggs are matured and ovulated during each menstrual cycle. For every egg that is released many more degenerate and are re-absorbed into the body. Eventually the ovary does not respond to the hormones that mature and release eggs and the woman experiences menopause. Because the eggs are present in the ovaries from birth, they age as the woman grows older, reducing their quality.
This is in contrast to male reproduction where sperm are constantly manufactured and replaced. The ageing of the eggs reduces their ability to be fertilized and to divide properly, leading to chromosomal abnormalities and a higher risk of miscarriage. Older women who receive eggs from a younger donor have a much higher chance of conceiving, confirming that the age of the eggs is crucial in achieving a pregnancy.
In IVF, age has a number of effects on the success of the treatment. The number of eggs collected is lower in older women and the quality of the embryos also generally decreases.
Higher doses of hormones are usually required in older women and there is also a higher risk of not having an egg collection due to poor or no response to the stimulating drugs. Unfortunately there is no way to reverse these effects of age on fertility.
Although age is not an absolute barrier to pregnancy, such factors as regular menstrual cycles or having had children before, do not necessarily indicate that pregnancy is possible in the late 30s and 40s.
For some women donor egg treatment may be the best chance to achieve a pregnancy. Information about the Donor Egg Program at Barbados Fertility Centre is available from your nurse coordinator, counsellor or clinician.
Fibroids
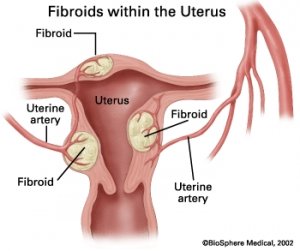
Fibroids are benign (non-cancerous) growths of the muscle of the uterus (womb). They are sometimes called myomas, fibromyomas or leiomyomas, but most people call them fibroids. Fibroids are common – around 20% of women get them.
Fibroids are most common in women in their 40s and 50s, towards the end of the reproductive years. They are more common in women of Afro-Caribbean origin, who also tend to be affected at a younger age. Fibroids are more likely to be found in women who have had no children or who only have one child. Obesity (being very overweight) is also associated with an increased risk of developing fibroids. They do not appear to run in families.
Fibroids grow very slowly and tend not to cause any problems or symptoms in younger women. They can cause symptoms as they grow bigger, but even so, at least half of all fibroids cause no problems at all.
Fibroids can be tiny or very large and a woman may have one or many. Their growth is stimulated by the hormone oestrogen, which is released from the ovaries during the reproductive years. Fibroids tend to become smaller after the menopause when oestrogen levels fall.
There are different types of fibroids, named according to where they are found:-
- Intramural fibroids are found within the muscular wall of the uterus.
- Subserosal fibroids grow outwards from the outside wall of the uterus. They can become very large.
- Submucosal fibroids grow from the inner wall of the uterus and can take up space inside the uterus. These account for only 5% of all fibroids.
The problems that fibroids may cause depend on their location. Fibroids are not the same as polyps. Polyps grow from the lining of the uterus (the endometrium) rather than from the underlying muscle (myometrium) as is the case with fibroids.
What are the symptoms?
Heavy periods
Up to half of all women with fibroids have heavy periods. In some cases this can lead to anaemia. Fibroids do not usually cause other problems with the menstrual cycle, such as bleeding between periods.
Pressure symptoms
Fibroids tend to enlarge the uterus. This may lead to lower abdominal discomfort or backache, or may press on the bladder causing symptoms such as needing to pass urine more often than normal. The uterus may also press on the rectum causing constipation. Some women experience pain or discomfort during sexual intercourse (dyspareunia) because of fibroids.
Problems with fertility
It is estimated that fertility problems are one of the presenting features in about ¼ of women with fibroids. There is a well-established relationship between the presence of fibroids and lower fertility or childlessness. When compared to other causes of infertility, however, they are a relatively uncommon cause, being implicated in only 3% of couples. It may be that a delay in having children (whether voluntary or involuntary) predisposes to the development of fibroids and this is more often an association rather than a causative feature.
Fibroids can affect the shape and internal environment of the uterus. They can make it more difficult to conceive but they only account for about 3% of the total cases of infertility.
Pain
Fibroids can cause discomfort because of pressure symptoms. Heavier periods can lead to worse period pains. Severe pain is quite rare but can occur if a fibroid grows on a stalk, which they twists (torsion) or if a fibroid outgrows its blood supply causing it to break down (red degeneration).
Diagnosis of fibroids
A doctor may suspect fibroids if he or she feels an enlarged uterus during a pelvic examination (an “internal”). An ultrasound scan is a useful way of confirming the present of fibroids. Here, a probe is placed on the woman’s lower abdomen and sound save signals are translated into pictures on a screen.
Fibroids can be detected by chance when women have ultrasound scans during pregnancy. Fibroids can also be detected by hysteroscopy, where a small telescope is passed through the cervix to view the inside of the uterus, or by laparoscopy, where a camera is passed into the abdomen through a keyhole incision and the outer wall of the uterus can be seen.
Treatment of fibroids
Fibroids don’t need to be treated if they cause no symptoms, or only mild symptoms, and if the diagnosis is certain. A repeat ultrasound scan may be carried out to ensure that the fibroids are not growing too rapidly.
Medicines
There are no long-term drug treatments that can “cure” fibroids. However, drugs are available that can help relieve the symptoms.
One group of drugs aimed at reducing the size of fibroids are called gonadotrophin releasing hormone analogues (GnRH analogues). These drugs stop the ovaries from producing hormones. Their effect is sometimes described as a “medical menopause” and they can cause menopausal symptoms such as hot flushes. However, there are increased risks of harmful side-effects such as osteoporosis (thinning of the bones) if they are given for more than six months. They may be used to control symptoms in women who are close to the menopause for whom symptoms may soon be about to improve anyway.
GnRH analogues are sometimes given before surgery on the uterus because shrinking the fibroids makes the operation easier.
Surgery
- Hysterectomy – this is a major operation to remove the uterus, usually via a “bikini-line” cut in the abdomen or, if the fibroids are not too large, via the vagina.
- Myomectomy – this is the removal of individual fibroids, leaving the uterus intact. It is usually only considered for women who still wish to have a baby. This may be done with through small cuts in the belly, using a laparoscope (keyhole surgery), but may require an open operation.
- Hysteroscopic resection – fibroids within the uterus can sometimes be removed during hysteroscopy using a hot wire loop (diathermy).
- Uterine artery embolisation – this is a new technique in which the blood supply to a fibroid is blocked, causing the fibroid to shrink. It is still undergoing research and is not yet widely available.
Fibroids are often detected at a routine scan during pregnancy. They do not necessarily cause any problems. However, there is an increased risk of miscarriage, premature labour and bleeding in women who have fibroids so it’s important to consider seeking specialist care from an obstetrician.
Most fibroids (around 80%) do not increase in size during pregnancy despite the extra hormones. Fibroids sometimes cause a severe abdominal pain during pregnancy if they break down (this is called red degeneration). The treatment for this is rest and painkillers.
Cancer arising in a fibroid is very rare. However, surgery to remove fibroids may still be recommended if there are symptoms of pain, bleeding and/or rapid growth of fibroids, especially in a post-menopausal woman.
Endometriosis
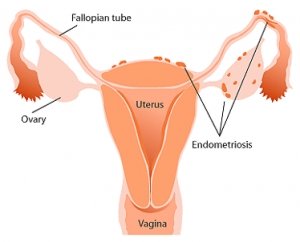
Endometriosis is a relatively common condition that can cause significant pain and suffering. Overall, between 3-10% of women aged between 15-45 years have endometriosis. In women who have difficulties conceiving, this rises to about 25-35%.
Endometriosis is small deposits of the womb lining that are located outside of the womb cavity. The most common place to find it is on the ovary, the back of the uterus and the uterosacral ligaments. It can also be found on the peritoneum, on the tubes or between the vagina and rectum (rectovaginal septum).
Each time that you have a normal period, so does this endometriosis, and this leads to cyclical swelling, stretching of tissues, inflammation and scarring. Eventually all the scarring and inflammation can lead to symptoms even when you’re not having a period.
The most common problems are:
- Pelvic pain
- Painful periods
- Pain during intercourse
- Infertility
The link between endometriosis and infertility is sometimes difficult to explain. When the disease is so bad that there is much scarring around the tubes, or there are ovarian cysts, it is not surprising that this interferes with normal fertility. But it is less clear how a few small spots of endometriosis might have a detrimental effect on attempts at pregnancy. Nevertheless, studies have found that endometriosis is more common in women who have difficulty conceiving.
Treatments for endometriosis
There are several options for treating endometriosis, and each has its place for different women’s disease. The options are as follows:
- No treatment at all
- Management of symptoms, e.g. using painkillers.
- Medical management, e.g. suppressing endometriosis, usually with GnRH agonists or the birth control pill.
- Conservative surgery, e.g. Laparoscopic surgery.
- Radical surgery, e.g. Hysterectomy.
Once the extent of your endometriosis has been evaluated your options would be reviewed and a specific course of treatment recommended.
Polycystic Ovarian Syndrome (PCOS)
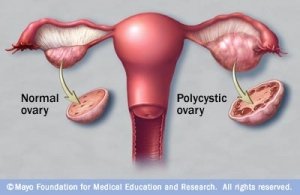
Polycystic ovarian syndrome is a condition in which there is a hormonal imbalance within the ovaries. It is a complex condition. In PCOS, the ovaries are bigger than average, and the outer surface of the ovary has an abnormally large number of smaller follicles (these are the sacs of fluid which grow around the egg in response to the stimulating hormones from the brain). In PCOS these follicles remain immature, which means that ovulation rarely happens and so the woman is often less fertile.
Women with PCOS may have the following problems:
1) infertility due to lack of ovulation
2) excessive body hair growth (hirsutism) due to an imbalance between hormones
3) irregular menstrual cycles and heavy bleeding (cycles which are either less than 21 days or more than 35 days apart) due to lack of ovulation
4) acne
5) obesity .
Some women with PCOS may have a higher than normal miscarriage rate if they become pregnant.
While it is not known if women are born with this condition, PCOS seems to run in families. Interestingly, when PCOS is passed down the man’s side of the family, the men are not infertile, but they do have a tendency to go bald before the age of 30.
Ongoing research is trying to clarify whether there is a clearly identifiable gene for PCOS. Women are also at a risk if they are overweight. Maintaining weight or body mass index (BMI) below a critical threshold is probably very important as weight loss improves hormonal abnormalities and improves the likelihood of ovulation and thus pregnancy.
The diagnosis of PCOS is made primarily on the woman's medical history and examination. The diagnosis can be confirmed on ultrasound or by measuring the woman's hormonal levels. A normal ultrasound or blood test result does not mean that the woman does not have the PCOS. Research suggests that women who do not have problems with their periods or have excessive hair growth can have ovaries, which on ultrasound, have the appearance of being polycystic.
The treatment of a woman with PCOS will depend on the presenting problems:
If a woman presents with irregular heavy bleeding, the oral contraceptive pill (OCP) is the treatment of choice, both to regulate the cycle and to prevent over growth of the endometrium (lining of the womb). Progesterone can also be given to replace what is not being produced monthly.
If hirsutism (excessive hair growth) is the problem then it can be treated using the OCP as well as with drugs that act against testosterone.
If infertility is the problem then clomiphene citrate (Clomid) given orally for 5 days early in the menstrual cycle may induce ovulation. Ovulation can be induced in 80% of women using Clomid and pregnancy rates approach those seen in the normal population (20-25% per month) provided that there are no other factors affecting fertility. If Clomid fails to induce ovulation or if the woman has tried Clomid for up to 6 cycles but has not become pregnant, follicle-stimulating hormone (FSH) at low doses may be given. Prior to using these drugs the treating doctor will want to make sure that the woman's Fallopian tubes are open and that her pelvis is normal.
These drugs are given by injection and when the woman uses these drugs she needs to be monitored using blood tests and ultrasounds to make sure that the drugs are not causing her to develop too many eggs. The aim when these drugs are used is to cause only one egg to develop (similar to in a natural cycle).
Nevertheless, the multiple pregnancy rate may be 20-30% with 80% of these multiple pregnancies being twin pregnancies.
Weight loss is also of paramount importance. The disease process may be reversed with loss of weight and there is also evidence that the higher miscarriage rate may decrease to that in the general population. A dietician may be required.
PCOS can lead to a resistance to insulin, leading to the body producing excessively high levels in an attempt to compensate. This higher level of insulin is known to cause abnormal cholesterol and lipid levels, obesity and an increased likelihood of diabetes. Metformin is a type of drug known as an “insulin-sensitising agent” which lowers the blood sugar level, in turn reducing the excessively high insulin.
There have been studies which show the use of insulin-sensitising drugs as a treatment for PCOS. These suggest that it may well be useful in several areas: helping weight reduction, normalizing blood cholesterol and improving irregular periods (70%) leading to ovulation. One study looking at ovulation in particular found that compared to no treatment, 34% of women ovulated taking Metformin (compared to 4% who did not receive it) and when this was combined with clomiphene it was as high as 90% (compared to 8% who only received clomiphene). The most common side effects during treatment on Metformin are diarrhoea, nausea, vomiting and abdominal bloating.
Alternatively, an operation called ovarian drilling can also be used to treat women with PCOS. This operation is usually reserved for women who want to be pregnant, and who have not ovulated on Clomid. In these women it may be used as an alternative to FSH. During this procedure the ovary is cauterized by drilling into it in a number of spots. We do not know exactly why this procedure works. If the operation is successful the effect may be long lasting.
In a small number of women, PCOS can be a very severe disease in that it can lead to the development of diabetes with all its complications. If the doctor suspects that the woman has this type of illness, she may need to undergo testing to make sure that she is not currently a diabetic. If diabetes is diagnosed then weight loss, diet and the possible use of tablets may be necessary.
Degrees & Positions

Scientific degrees
- Phd degree of Obstetrics and gynecology, Faculty of Medicine, Alexandria University, November 2007.
- Fellowship of assisted reproductive techniques, Universiatsklinikum Schleswig-Holstein, Klinik für Frauenheilkunde und Geburtshilfe,Kampus Lübeck, Germany, 2004.
- The European university diploma of advanced gynecological laparoscopy, University of Auvergne, France, 2004.
-
Master degree of Obstetrics and gynecology, Faculty of Medicine, Alexandria University, November 2000. (Excellence with the degree of honor).
-
M.B.B.Ch, Faculty of Medicine, Alexandria University, October 1995 (Excellence with the degree of honor).
Appointments
- Assistant Professor of Obstetrics and Gynecology , Faculty of Medicine,University of Alexandria, Egypt, 2014.
-
Senior embryologist, Agial IVF center, 2009.
-
Senior embryologist, Miami IVF center, 2005- 2009.
-
Consultant of Obstetrics &Gynecology, Gherian University Hospital, Libya, 2008
-
Lecturer of Obstetrics and Gynecology, Faculty of Medicine, University of Alexandria, Egypt, February 2008.
-
Reviewer, Journal of Endocrinological Investigation, published for the Italian Society of Endocrinology by Editrice Kurtis.
-
Research Fellow and Clinical staff Specialist, School of Health Sciences, Vaxjo University, Sweden, 2005.
-
Clinical Fellow, Universitatsklinikum Schleswig-Holstein, Klinik für Frauenheilkunde und Geburtshilfe,Bereich für Reproduktionsmedizin, Kampus Lübeck,Germany, 2004.
-
Editorial assistant in the Egyptian post menopause society newsletter.
-
Assistant Lecturer of Obstetrics and Gynecology in El Shatby Maternity University Hospital, University of Alexandria, Egypt, 23-4-2001 till February 2008.
-
Demonstrator of Obstetrics and Gynecology in El Shatby Maternity University Hospital, University of Alexandria, 10-1-2001till 21-4-2001.
-
Resident Registrar of Obstetrics and Gynecology in El Shatby Maternity University Hospital, University of Alexandria, 10-12-1997 till 9-12-2000.
-
General practitioner in the Egyptian Ministry of Health Hospitals, 1-3-1997 till 9-12-1997.
-
House Officer in the Alexandria University Hospitals, 1-3-1996 till 28-2-1997.
Scientific Societies
- Member of the European Society of Human Reproduction and Embryology (ESHRE).
- Member of the Middle East Fertility Society (MEFS).
- Member of the Egyptian association for gynecological laparoscopies (EAGL).
- Member and editorial assistant in the Egyptian post menopause society newsletter.
- Founder Member of the Reproductive Biology and Molecular Endocrinology Interest Group in the Egyptian Fertility and Sterility Society.